

Summary
Some clinically important members of the Brucella family include Brucella abortus, Brucella melitensis, Brucella canis and Brucella suis. [1]
Some clinically important members of the Brucella family include Brucella abortus, Brucella melitensis, Brucella canis and Brucella suis. [1]
Staining and microbiologic features:
- Facultative intracellular organisms [2]
- Aerobic coccobacilli that are gram-negative and non-motile [1]

Brucella by Anna Carla Silva Cunha is licensed under CC BY-SA 4.0.
- Growth of certain brucella strains (such as B. abortus) requires CO2. [3]
- Brucella strains infecting humans can test positive for catalase and oxidase [3]
- Non-encapsulated and does not form spores [1,3]
- Brucella colonies exhibit a remarkable versatility in their morphology. Based on O antigen within the cell wall lipopolysaccharide (LPS), they can assume two distinct forms: smooth, characterized by translucency and homogeneity, and rough, distinguished by opacity, granularity, or a sticky texture.

PIXNIO-38568-4206×3153 by Walker16 is licensed under CC BY-SA 4.0.
Antibodies directed against one specific form lack cross-reactivity against the other form.[1]
Virulence:
- Many Brucella strains can metabolize erythritol. Some animal tissues and organs, such as the placenta, uterus, and epididymis, have high erythritol content. Therefore, brucella shows tropisms for these organs. [1,4]
- The greatly diminished virulence observed after the reversion of smooth strains to the rough morphology underscores the importance of the O chain in the smooth lipopolysaccharide (LPS) as a crucial marker for virulence. [1]
- Absence of detectable exotoxin [1]
Transmission:
- Direct contact while handling infected animal tissues such as placenta or meat [5]
- Consuming contaminated animal products (e.g., dairy products made from unpasteurized milk) [3,5]
- Breathing in contaminated droplets [1,3]
Geographic distribution/Incidence:
- Worldwide occurrence. However, the disease is less common in the USA due to animal vaccination and milk pasteurization. [5]
Diseases:
- Brucellosis: Some other names used for this disease include Bang disease, Malta fever, Mediterranean remittent fever, and undulant fever. After entering the body, the macrophages and monocytes phagocytose these organisms and carry them to other body parts, such as lymph nodes, spleen, liver, and bone marrow. Brucella survives in these phagocytic cells and causes granulomatous inflammation. [1,3] The affected patient can present with undulant fever (intermittent fever that peaks during the afternoon and subsides during the night) and some nonspecific symptoms like malaise, drenching sweats, fatigue, nonproductive cough, and muscle pain. Lymphadenopathy and splenomegaly are also possible. Brucella can also result in hepatitis and osteomyelitis. [6,7]
- Brucella can be a potential weapon for biological warfare. [1]
Diagnostic testing:
- Specimens from bone marrow, blood, lymph nodes, or liver are obtained and cultured on enriched blood agars. Allow a 2-week incubation period for blood cultures before deeming them -ve. [7,8]
- A skin test using brucellergin can detect brucella exposure. However, it cannot provide definitive confirmation of active brucellosis. [8]
- Agglutination tests can detect IgG antibodies against brucella. There is an indication of an active infection when IgG agglutinin titers surpass 1:80. [7]
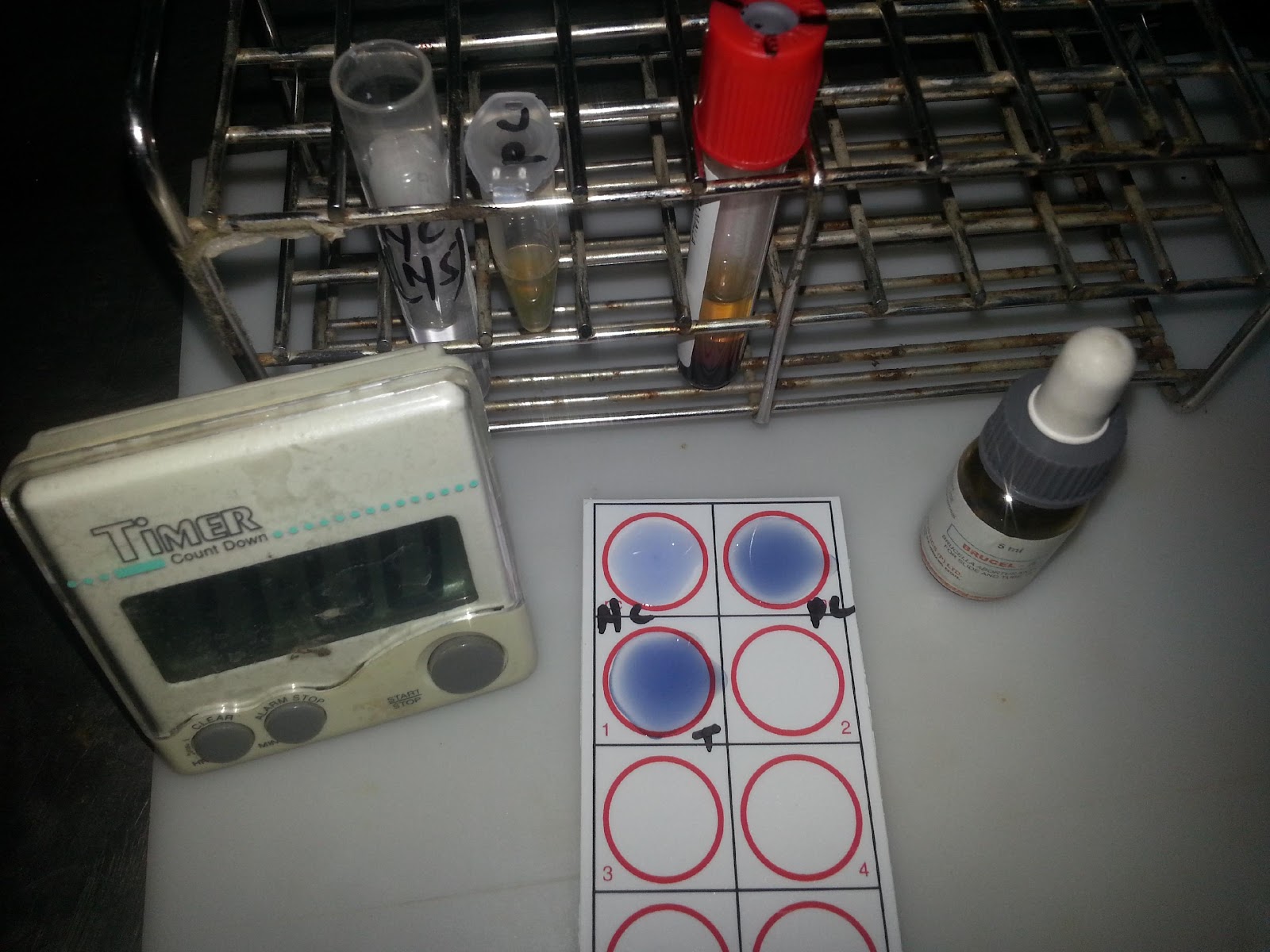
Brucella Agglutination Test by Ajay Kumar Chaurasiya is licensed under CC BY-SA 4.0.
- Some blocking antibodies, IgA type, can disrupt the agglutination reactions of both IgG and IgM. As a consequence, serologic test outcomes appear negative at low serum dilutions. These blocking antibodies can be identified through the Coombs antiglobulin method [7]
- ELISA [9]
References:
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 293)
- CMMRS edition 6, 2016-17 (page no: 109)
- Jawetz, Melnick, & Adelberg’s Medical Microbiology Twenty-Seventh Edition (page no: 269)
- CMMRS edition 6, 2016-17 (page no: 108)
- CMMRS edition 6, 2016-17 (page no: 106)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 294)
- Jawetz, Melnick, & Adelberg’s Medical Microbiology Twenty-Seventh Edition (page no: 270)
- CMMRS edition 6, 2016-17 (page no: 107)
- Jawetz, Melnick, & Adelberg’s Medical Microbiology Twenty-Seventh Edition (page no: 271)