

Summary
Some clinically important members of the Chlamydiaceae family include Chlamydia trachomatis, Chlamydophila pneumoniae, and Chlamydophila psittaci [1].
Some clinically important members of the Chlamydiaceae family include Chlamydia trachomatis, Chlamydophila pneumoniae, and Chlamydophila psittaci [1].
Microbiologic features:
- Chlamydia is an obligate intracellular organism [2].
- It cannot produce ATP and uses an ATP/ADP translocator to obtain ATP from its host [2].
- It has a gram-negative cell wall. In contrast to other Gram-negative bacteria, its cell wall is devoid of peptidoglycan and muramic acid [2].
- The Chlamydia life cycle has two distinct forms: elementary bodies and reticulate bodies/initial bodies.
- Elementary bodies are infectious and metabolically inactive. This form has abundant disulfide bond cross-linkages and, therefore, can survive in an extracellular environment. These elementary bodies cannot undergo replication but are responsible for the initial attachment to host cells and promoting endocytosis [3].
- Reticulate bodies are metabolically active. Upon entering host cells, elementary bodies disrupt the fusion of phagosomes with lysosomes. Subsequently, they increase in size, boost RNA production, and generate new elementary bodies. These reticulate bodies lack extensive cross-linking of membrane proteins. The reticulate bodies then transform into elementary bodies, which can later exit the host cells. [3,4]
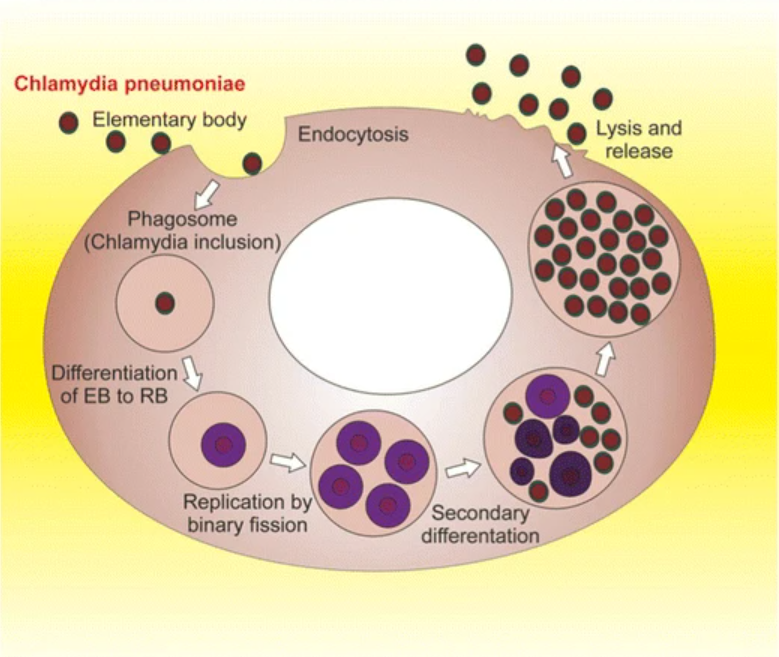
12035 2012 8320 Fig3 HTML by Giovanna De Chiara, Maria Elena Marcocci, Rossella Sgarbanti, Livia Civitelli, Cristian Ripoli, Roberto Piacentini, Enrico Garaci, Claudio Grassi, Anna Teresa Palamara is licensed under CC BY 2.5.
- Chlamydia trachomatis and Chlamydia psittaci can contain plasmid DNA, while it is absent in Chlamydia pneumoniae. Iodine staining reveals glycogen inclusion in Chlamydia trachomatis and its absence in the other two species. Additionally, among the three, Chlamydia trachomatis is susceptible to sulfonamides [5].
Virulence:
- It uses a type 3 secretion system to insert virulent proteins into the host cells [4].
- The absence of muramic acid in their cell walls confers resistance against lysozyme [6].
- The organism is non-motile and lacks pili and exotoxins [6].
- Chlamydia has lipopolysaccharides in its cell wall; however, unlike other gram-negative organisms, its endotoxin activity is weak [5].
Transmission and reservoirs:
Chlamydia trachomatis: Transmission can occur via exposure to infected fluids, facilitated by different vectors such as droplets, hands, contaminated clothing, and flies. Additionally, transmission can result from respiratory droplets and fecal contamination, particularly in regions with high endemicity, where the risk is high due to poor hygiene. In adults, transmission is feasible through autoinoculation and oral-genital contact. Mother-to-child transmission is also possible during childbirth from an infected mother [7].
Chlamydophila psittaci: Transmission is possible through inhalation of contaminated bird secretions such as dried feces, urine, or respiratory fluids [8].
Chlamydophila pneumoniae: Person-to-person transmission can occur through respiratory droplets.
Humans serve as reservoirs for Chlamydia trachomatis and Chlamydophila pneumoniae, while birds act as reservoirs for Chlamydophila psittaci [9,10].
Diseases and complications:
Chlamydia trachomatis can cause trachoma, inclusion conjunctivitis, infant pneumonia, urethritis, cervicitis, epididymitis, lymphogranuloma venereum, and pelvic inflammatory disease.
- Trachoma: Chlamydia trachomatis serotypes A, B and C can cause trachoma. It is the most frequent cause of preventable blindness in the world [11]. The patient may present with signs and symptoms of follicular conjunctivitis. As the disease progresses, scarring exerts traction on the eyelid, resulting in inverted eyelids. The inward-turned eyelashes can then lead to corneal ulceration and subsequent blindness.
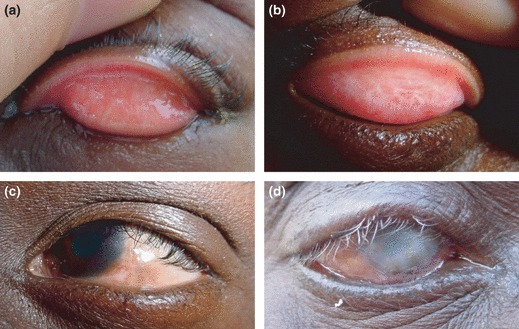
Trachoma 1 by Hu VH, Harding-Esch EM, Burton MJ, Bailey RL, Kadimpeul J, Mabey DC. is licensed under CC BY 2.5.
Recurrence is common in children residing in trachoma-endemic areas and immigrants with childhood-acquired infections [7].
- Lymphogranuloma venereum: Chlamydia serotypes L1, L2, and L3 cause lymphogranuloma venereum [11]. The patient can initially develop a painless papule or ulcer in the genital area. After spontaneous healing of the initial lesion, the patient develops lymphadenitis of regional lymph nodes. Subsequent rupture of these lymph nodes can form draining fistulas. Proctitis can also develop in women and homosexual men. Untreated cases can progress to elephantiasis of the genitals and rectal strictures [12, 13].

Lymphogranuloma venerum – lymph nodes by Herbert L. Fred, MD and Hendrik A. van Dijk is licensed under CC BY 2.0.
- Inclusion conjunctivitis: Chlamydia serotypes D-k can cause inclusion conjunctivitis. Newborns will present with conjunctivitis with purulent ocular discharge a few days after birth. Evaluation of conjunctival cells in affected patients will reveal characteristic basophilic intracytoplasmic inclusion bodies [6].
- Nongonococcal urethritis: Chlamydia serotypes D-k can also cause nongonococcal urethritis [11]. The patient can present with dysuria and urethral discharge [14]. Unlike gonococcal infection, gram-negative intracellular diplococci are absent.
- Pelvic inflammatory disease: Cervicitis infection can spread to other reproductive organs. Patients can present with fever, lower abdominal pain or pelvic pain, painful intercourse, and vaginal discharge. The Chandelier sign during the pelvic examination can confirm cervical motion tenderness. Subsequent scarring in untreated cases can cause infertility and ectopic pregnancy. As Chlamydia infection can be asymptomatic or manifest with mild symptoms, the disease may go unnoticed, eventually leading to complications such as infertility [14].
- Infant pneumonia: Newborn will present with respiratory symptoms such as difficulty breathing, tachypnea, and cough. Laboratory testing will show elevated IgM levels [15].
- Some other possible complications of chlamydia trachomatis infection include chronic pelvic pain, Fitz-Hugh-Curtis syndrome, and Reiter’s syndrome [6].
Chlamydia psittaci causes psittacosis, and the patient may present with a cough and some nonspecific symptoms, including headache, fever, chills, and muscle aches [8].
Chlamydophila pneumoniae causes atypical pneumonia. Some studies propose an association between C. pneumoniae and atherosclerosis. Nevertheless, the precise involvement of C. pneumoniae in the pathogenesis of atherosclerosis remains unclear [16].
Diagnostic testing:
Chlamydophila pneumoniae and chlamydia psittaci:
- Serodiagnosis is possible through micro immunofluorescence (MIF) and complement fixation tests. These tests will show high antibody levels [17].
- Inclusion bodies in C. pneumoniae lack glycogen and remain unstained with iodine [17,18].
Chlamydia trachomatis:
- Precise specimen collection is crucial for accurate Chlamydia diagnosis. While pus and vaginal exudate may be readily available, their low organism yield necessitates preferential acquisition from sites harboring columnar or squamocolumnar epithelium, namely the endocervix, urethra, rectum, oropharynx, and conjunctiva. This prioritization aligns with Chlamydia’s preference for these cell types [19].
- Nucleic acid amplification tests (NAATs) have high sensitivity and specificity for diagnosing chlamydia infections [19].
- Iodine staining of conjunctival cells in patients with inclusion conjunctivitis will reveal glycogen-containing intracytoplasmic inclusions [6].
- Unlike many bacteria, Chlamydia trachomatis cannot replicate on standard laboratory media. Instead, specific culture systems, such as those incorporating McCoy cells or chick yolk sacs, provide a suitable environment for its growth [6].
- PCR is helpful for diagnosis in patients with urethritis [6].
- Serodiagnosis is possible through micro immunofluorescence (MIF) and complement fixation tests. These tests will show high antibody levels [6].
- Frei test (not commonly used) for lymphogranuloma venereum [6]
References:
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 348)
- CMMRS edition 6, 2016-17 (page no: 110)
- CMMRS edition 6, 2016-17 (page no: 111)
- Jawetz, Melnick, & Adelberg’s Medical Microbiology Twenty-Seventh Edition (page no: 351)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 349)
- CMMRS edition 6, 2016-17 (page no: 123)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 351)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 355)
- CMMRS edition 6, 2016-17 (page no: 122)
- CMMRS edition 6, 2016-17 (page no: 124)
- CMMRS edition 6, 2016-17 (page no: 112)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 352)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 357)
- CMMRS edition 6, 2016-17 (page no: 114)
- CMMRS edition 6, 2016-17 (page no: 113)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 354)
- CMMRS edition 6, 2016-17 (page no: 125)
- Jawetz, Melnick, & Adelberg’s Medical Microbiology Twenty-Seventh Edition (page no: 358)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 353)