

Summary
Leptospira interrogans is the causative agent of leptospirosis, a ubiquitous zoonotic disease. In the United States, the majority of cases occur in Hawaii, with seasonal peaks coinciding with increased recreational activities during warmer months [1].
Leptospira interrogans is the causative agent of leptospirosis, a ubiquitous zoonotic disease. In the United States, the majority of cases occur in Hawaii, with seasonal peaks coinciding with increased recreational activities during warmer months [1].
Virulence and microbiologic features:
- Leptospira interrogans is a spirochete with a distinctive spiral shape. It may exhibit an ‘ice tongs’ appearance characterized by distinctive hooks at one or both ends of the bacterium [2].
- As an obligate aerobe, it thrives best in the presence of oxygen, demonstrating optimal growth between 28 and 30 °C [3].
- It has a broad range of animal reservoirs, including dogs, cats, livestock, and wild animals, with humans serving as incidental hosts [1]
- It uses periplasmic flagella for movement [4].
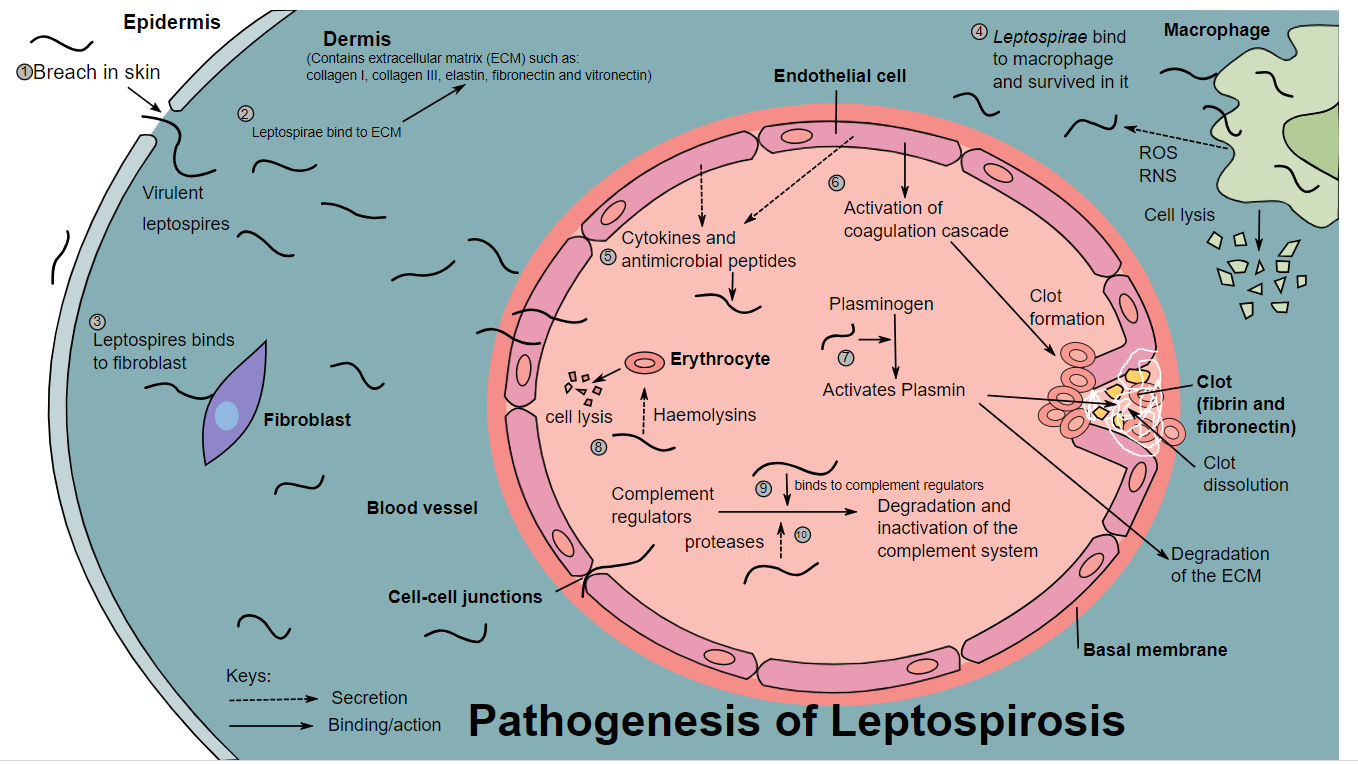
Pathogeneis of leptospirosis by Cerevisae is licensed under CC BY-SA 4.0.
Transmission:
- Human exposure to Leptospira interrogans often occurs through contact with contaminated water sources, such as during recreational activities. In addition, handling infected animals or animal tissues poses a potential risk of occupational exposure. Also, the organism can enter through compromised skin and mucosal surfaces [1,4].
Diseases and Complications:
- Leptospirosis: In the initial stage of infection, the bacterium infiltrates the bloodstream and cerebrospinal fluid (CSF), leading to a sudden rise in body temperature, accompanied by symptoms like severe headaches, general discomfort, and myalgias. Another distinctive indicator is conjunctival suffusion, characterized by redness in the eyes without discharge and increased sensitivity to light [2,5].

Conjunctival suffusion of the eyes due to leptospirosis by Daniel Ostermayer, from Houston, Texas, United States is licensed under CC BY 4.0.
Following approximately seven days of the initial infection phase, a brief afebrile period ensues before the recurrence of initial symptoms. This second phase coincides with the emergence of IgM antibodies. Meningitis may develop, and most patients exhibit an elevated white blood cell count in cerebrospinal fluid (CSF).
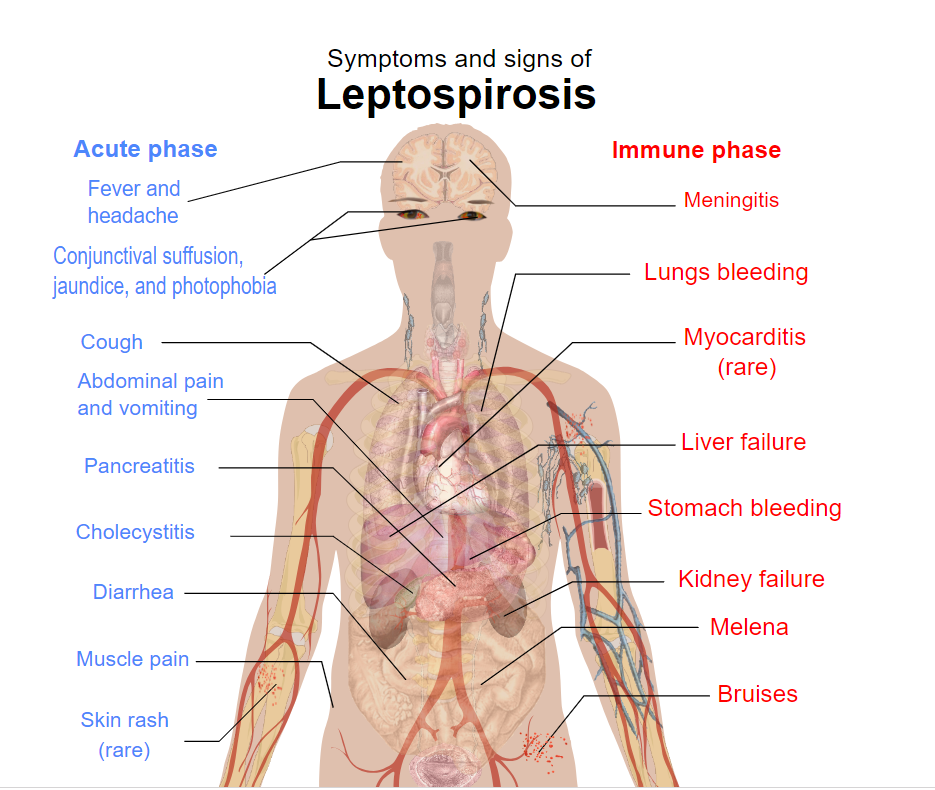
Signs and symptoms of leptospirosis by Cerevisae is licensed under CC BY-SA 4.0.
- Weil disease, also known as icterohemorrhagic leptospirosis, represents a severe and potentially life-threatening form of leptospirosis and is characterized by manifestations such as multiorgan failure involving both renal and liver systems, as well as anemia and hemorrhage [5,6].

Diffuse pulmonary haemorrhages of the lungs infected by leptospirosis by Nuwan Ranawaka, Vijayabala Jeevagan, Panduka Karunanayake and Saroj Jayasinghe is licensed under CC BY 2.5.
Diagnostic Testing:
- Culture: Leptospira isolation during the initial phase is possible through blood and CSF cultures. In the second phase and ensuing weeks, urine becomes the preferred sample for culture [2].
- Darkfield microscopy (not advised) [6]
- Nucleic acid-based testing, such as PCR [7]
- Antibody detection is feasible through various methods, including the microscopic agglutination test (MAT) exclusively conducted in reference laboratories, indirect hemagglutination, slide agglutination, or enzyme-linked immunosorbent assay (ELISA) [7].
References:
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 332)
- CMMRS edition 6, 2016-17 (page no: 137)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 331)
- CMMRS edition 6, 2016-17 (page no: 140)
- First Aid for USMLE step 1, 2021 edition (page no: 147)
- CMMRS edition 6, 2016-17 (page no: 141)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 333)