

Summary
Mycobacterium tuberculosis is the causative agent for tuberculosis. Individuals who are not born in the U.S., the homeless, substance abusers, prisoners, and those with compromised immune systems, such as those living with HIV, face an elevated risk of infection [1].
Mycobacterium tuberculosis is the causative agent for tuberculosis. Individuals who are not born in the U.S., the homeless, substance abusers, prisoners, and those with compromised immune systems, such as those living with HIV, face an elevated risk of infection [1].
Staining and microbiologic features:
- Mycobacterium tuberculosis is an acid-fast organism because the abundance of lipids in its cell wall prevents decolorization by acid or alcohol during the staining process [2,3].
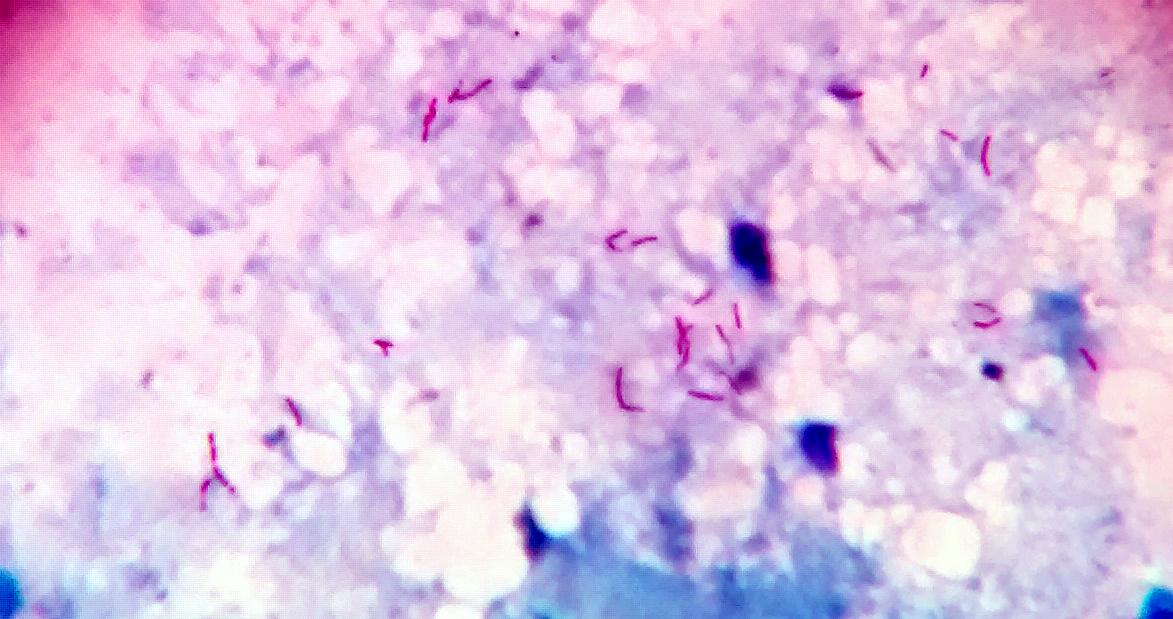
Acid fast bacilli in sputum smear by Microrao is licensed under CC BY-SA 4.0.
- It is an obligate aerobe because it needs oxygen for its growth and metabolic activities [4].
- It is a non-spore-forming rod and is nonmotile [3].
- It is nonmotile and lacks a capsule [5].
- It also tests positive for catalase [5].
Virulence:
- Cord factor is produced by virulent strains of M. tuberculosis, allowing for parallel growth of the bacteria and facilitating the formation of bacterial cell cords [2]. Cord factor could also impair neutrophil migration and induce the release of tumor necrosis factor (TNF), potentially leading to weight loss [6].
- Sulfatides produced by M. tuberculosis inhibit the fusion of the phagosome with the lysosome and thus aid in the facultative intracellular growth of the bacterium [6].
- Wax D enhances the immune response by acting as an adjuvant and can elicit the cellular immune response [6].
- Mycobactin, a siderophore, assists the organism in extracting iron [5].
- It lacks pilli, exotoxins, and endotoxins [5].
- IL-12 and TNF-α released by macrophages promote the differentiation of T cells into TH1 cells, leading to the release of IFN-γ. This interferon promotes the effective fusion of phagosomes with lysosomes and the efficient killing of phagocytosed bacteria. Insufficient production of IFN-γ or TNF-a (as in patients taking TNF-a inhibitors) heightens susceptibility to severe infections [7]. Granulomas serve to contain the organism. However, if the bacterial load is high, the bacteria may persist in a dormant state for an extended period and potentially reactivate in situations such as old age or immunosuppression [5].
Transmission:
- Airborne Transmission: Inhaling aerosols carrying infectious M. tuberculosis [4].
Diseases and complications:
- Primary tuberculosis: Patients can be either asymptomatic or may present with fever, weight loss, night sweats, productive cough, and possibly cavitary lesions on chest X-ray [8,9].
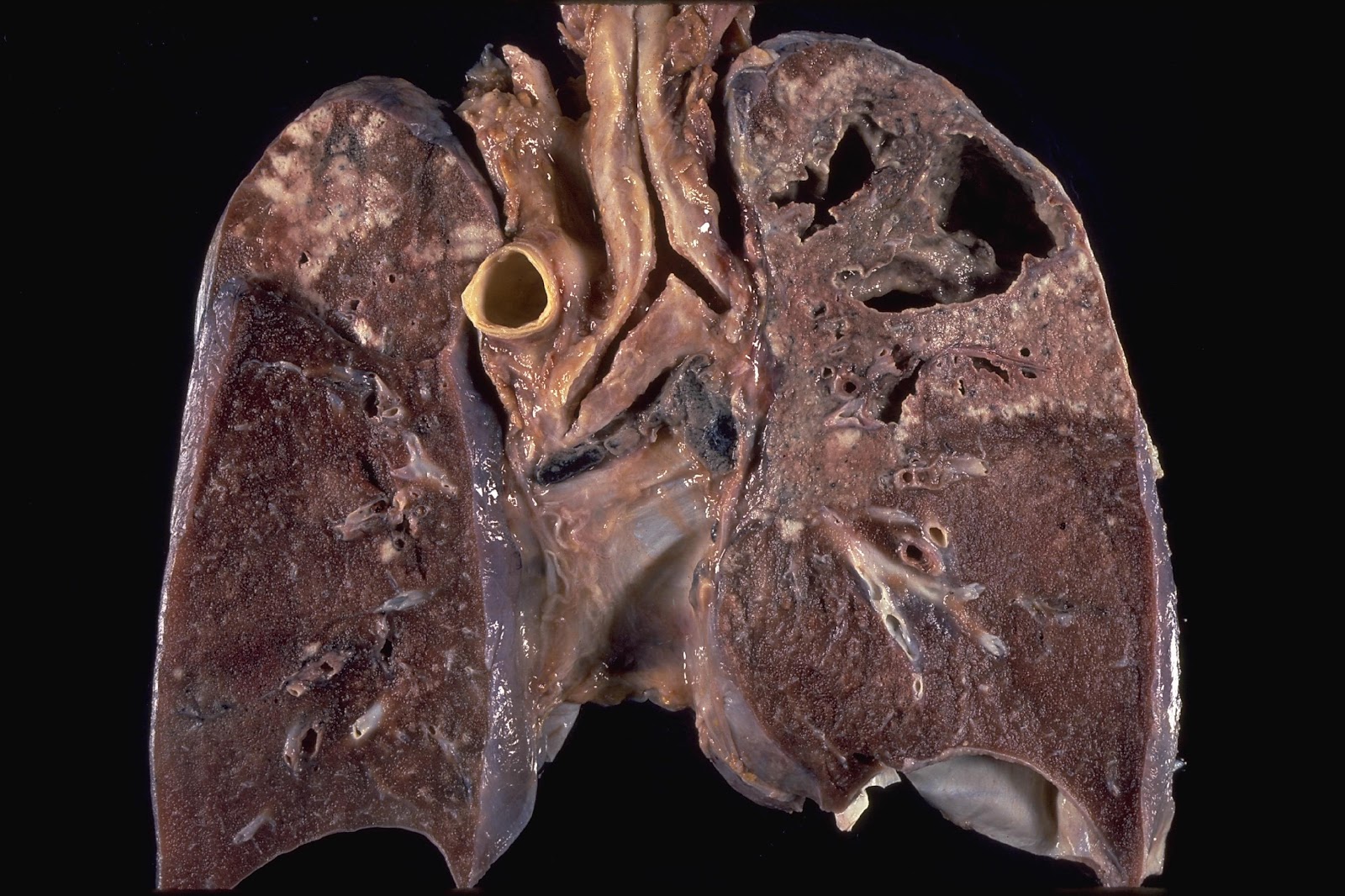
File:Cavitary tuberculosis.jpg by Yale Rosen is licensed under CC BY-SA 2.0.
- Secondary tuberculosis: The risk of reactivation is high in immunocompromised patients such as in AIDS patients [9].
- Pott’s disease: It is a form of extrapulmonary tuberculosis that affects the spine [10].
- Miliary tuberculosis: A disseminated form of tuberculosis (TB) characterized by the widespread dissemination of tiny granulomas throughout the body, affecting various organs [10].

File:Chest radiograph of miliary tuberculosis 2.jpg by Benjamín Herreros, Isabel Plaza, Rebeca García, Marta Chichón, Carmen Guerrero and Emilio Pintor is licensed under CC BY 4.0.
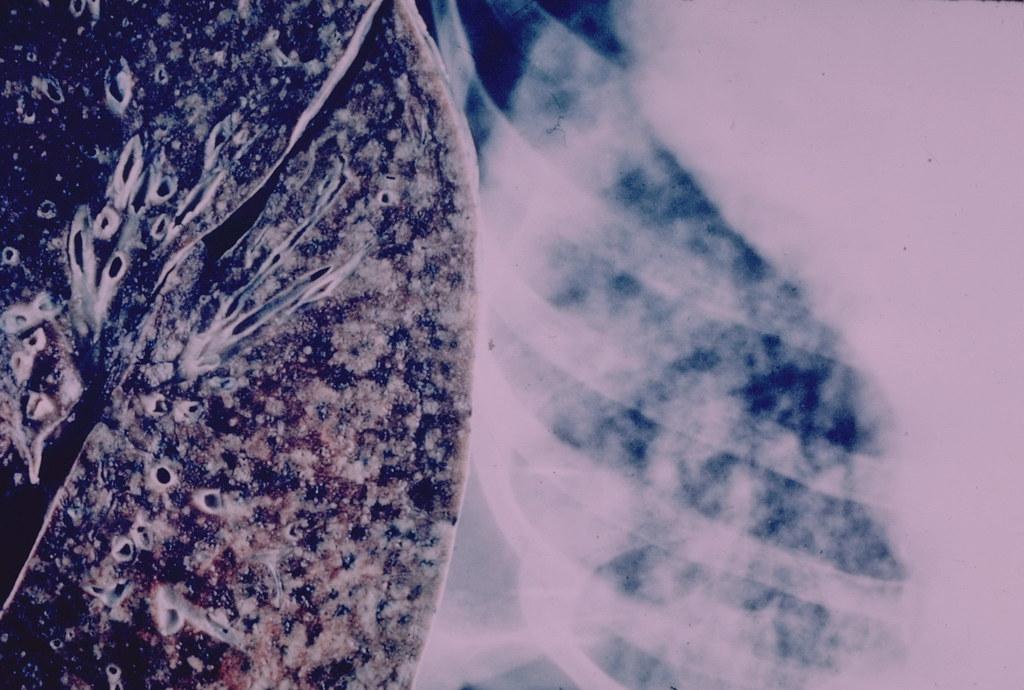
“Lung – Miliary tuberculosis” by Pulmonary Pathology is licensed under CC BY-SA 2.0.
- Scrofula: An extrapulmonary manifestation due to the involvement of cervical lymph nodes [10].
Diagnostic testing:
- Staining, especially with Ziehl-Neelsen, will reveal acid-fast rods in the specimen [3].
Acid fast bacilli in sputum smear by Microrao is licensed under CC BY-SA 4.0.
- Faster detection is possible by culturing the organism on bactec radiometric culture [11].
- Interferon-gamma release assay (IGRA) is particularly useful in individuals who have received the BCG vaccination [12].
- Tuberculin skin test: An induration of a certain size is considered positive. The size cutoff for a positive result varies:
- An induration of ≥ 5 mm is considered positive in patients with compromised immune system [11,13].
- An induration measuring ≥ 10mm is considered positive in some patients if there are additional risk factors. These factors include being a healthcare worker, having a chronic disease such as diabetes or renal failure, or originating from a country with a high TB incidence [11,13].
- Induration of ≥ 15mm is considered positive in all other patient groups [11,13].
- False positive results can occur in patients who received the BCG vaccine, and false negative results are possible in immunocompromised and malnourished patients [13].
- Rapid detection is possible through Gene Xpert MTB/RIF [14].
- Imaging studies include chest x-rays and CT scans.
References:
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 119)
- CMMRS edition 6, 2016-17 (page no: 142)
- Jawetz, Melnick, & Adelberg’s Medical Microbiology Twenty-Seventh Edition (page no: 309)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 222)
- CMMRS edition 6, 2016-17 (page no: 150)
- CMMRS edition 6, 2016-17 (page no: 143)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 221)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 223
- CMMRS edition 6, 2016-17 (page no: 145)
- CMMRS edition 6, 2016-17 (page no: 146)
- CMMRS edition 6, 2016-17 (page no: 151)
- Jawetz, Melnick, & Adelberg’s Medical Microbiology Twenty-Seventh Edition (page no: 313
- CMMRS edition 6, 2016-17 (page no: 144)
- CMMRS edition 6, 2016-17 (page no: 147)