

Summary
Rickettsia genus includes the spotted fever group (Rickettsia rickettsii, Rickettsia conorii, Rickettsia sibirica) and the typhus group (Rickettsia prowazekii, Rickettsia typhi, Orientia tsutsugamushi) [1,2].
Rickettsia genus includes the spotted fever group (Rickettsia rickettsii, Rickettsia conorii, Rickettsia sibirica) and the typhus group (Rickettsia prowazekii, Rickettsia typhi, Orientia tsutsugamushi) [1,2].
Staining and microbiological features:
- Pleomorphic coccobacilli [3]
- Although it is a Gram-negative organism, it exhibits poor Gram staining due to scant peptidoglycan content [4].
- It is an obligate intracellular pathogen (i.e., Rickettsia relies on host metabolic machinery to meet its energy/ATP requirements) [5].
- Reservoirs for the rickettsiae of spotted fever group, Orientia tsutsugamushi, and Rickettsia typhi are rodents [2]. Reservoirs for Rickettsia prowazekii include humans and flying squirrels [5].
Virulence and pathogenicity:
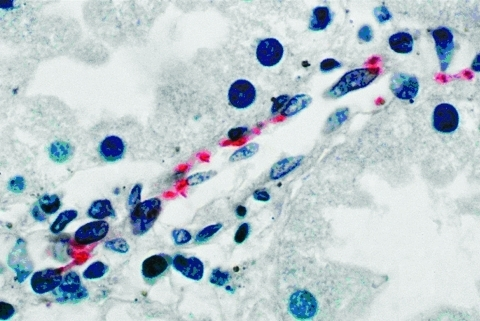
(Rickettsia rickettsii in the endothelial cells on immunohistochemical staining)
PMC3035541 03-0193-F2 by Márcio Antonio Moreira Galvão, J. Stephen Dumler, Cláudio Lísias Mafra, Simone Berger Calic,Chequer Buffe Chamone, Gracco Cesarino Filho, Juan Pablo Olano,David H. Walker is marked with CC0 1.0.
- OmpA and OmpB are surface proteins that help the organism attach to target cells. After the organism is phagocytosed, it escapes the phagosome through the action of phospholipase, which disrupts the phagosome membrane [3, 4]. Subsequently, it survives and replicates in the cytoplasm [6].
- Cells infected with Orientia and rickettsiae of the Spotted fever group consistently liberate these organisms via extended cytoplasmic projections, while the typhus group aggregates within the cell up to the point where the cell membrane ruptures and results in the cell death and the subsequent release of bacteria [4].
- It uses an ATP/ADP translocator to get ATP from the host [8].
- It is susceptible to heat, bactericidal chemicals, and drying [3].
- It does not produce exotoxins [9].
Transmission:
- Tick-borne transmission: Dermacentor andersoni (wood tick) transmits Rickettsia rickettsii in the western U.S, and Dermacentor variabilis (dog tick) is responsible for transmitting Rickettsia rickettsii in the eastern U.S [5].

Rocky mountain-spotted fever tick, rocky mountain wood tick, tique d’anderson by Tobi (he/him) is licensed under CC BY 4.0.

Female Dog Tick by NIAID is licensed under CC BY 2.0.
- Louse-borne transmission: Pediculus corporis (human body louse) transmits Rickettsia prowazekii [5].

Human body louse by Ark. Agricultural Experiment Station is licensed under CC BY 2.0.
- Flea-borne transmission: Xenopsylla cheopis (Rat flea) transmits Rickettsia typhi [5].

Xenopsylla rat flea (plague flea) by Michael Wunderli is licensed under CC BY 2.0.
- Mite-borne transmission: Chiggers (Mite larvae) transmit rickettsia tsutsugamushi [5].
Diseases and complications:
- Rocky Mountain spotted fever: Rickettsia rickettsii causes Rocky Mountain spotted fever (more frequently in the southeastern U.S.). The patient can present with a rash that tends to begin on the wrists and ankles and then spreads to the trunk and extremities, including the palms and soles. Some associated signs and symptoms include fever, headache, and conjunctivitis [10].
- Epidemic typhus: Rickettsia prowazekii causes epidemic typhus. The patient can present with fever, headache, and rash. The rash of the epidemic typhus begins on the upper trunk and then quickly spreads to the remaining body. Unlike Rocky Mountain spotted fever, it does not involve the face, palms, and soles [11]. Some patients may also experience delirium, and compromised blood supply due to intravascular clotting can lead to gangrenous necrosis in the hands and feet [11, 12].

Epidemic Typhus. Macular rash 1 by Georg Jochmann is licensed under CC BY-SA 4.0.
- Brill-Zinsser disease: After an initial infection of epidemic typhus, Rickettsia prowazekii can remain dormant in the body for an extended period. Brill-Zinsser disease occurs when the latent Rickettsia prowazekii reactivates, leading to a milder disease. Diagnostic testing will reveal a swift initial increase in IgG antibodies, in contrast to the primary infection, where IgM levels increase [12].
- Endemic typhus/murine typhus: Rickettsia typhi causes endemic typhus, and the affected patient can present with fever, rash, and headache [9].
- Scrub typhus: O. tsutsugamushi causes scrub typhus, and the patient can present with fever, headache, and eschar at the site of chigger bite. A rash may ensue following these symptoms [13].

File:Scrub typhus eschar.jpg by Paula Santibáñez, Ana M. Palomar, Aránzazu Portillo, Sonia Santibáñez and José A. Oteo is licensed under CC BY-SA 3.0.
- Rickettsialpox: Rickettsia akari is responsible for causing rickettsialpox, a self-limited condition. Patients may initially present with a papule at the site of the mite bite. This papule subsequently evolves into a vesicle. Within days, fever and headache ensue, and additional vesicles appear across the body, resembling the presentation of chickenpox [10].
Diagnostic testing:
- Microscopy: Giemsa or Gimenez stains and fluorescent-labeled antibodies can be helpful in visualizing rickettsia.
- Weil-Felix test: It relies on detecting antibodies in the patient’s blood that react with surface antigens of some Proteus species. Some antigens of Proteus Mirabilis, such as OX-19, OX-2, and OX-K, share some cross-reactivity with antigens of Rickettsia. Positive reactions in the test could indicate exposure to either rickettsia or the specific Proteus species used [14,15]. Positive reactions with OX-19 and OX-12 indicate Rickettsia rickettsii infection. OX-19 is positive for Rickettsia prowazekii and Rickettsia typhi infections. OX-K is positive for Orientia tsutsugamushi infection [9]. OX-K, OX-19, and OX-12 are negative for Rickettsia akari infection [6].
- Serological testing also includes indirect immunofluorescence and enzyme immunoassays [16].
- Culture (not widely used) [17]
References:
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 339)
- Jawetz, Melnick, & Adelberg’s Medical Microbiology Twenty-Seventh Edition (page no: 342)
- Jawetz, Melnick, & Adelberg’s Medical Microbiology Twenty-Seventh Edition (page no: 341)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 340)
- CMMRS edition 6, 2016-17 (page no: 124)
- CMMRS edition 6, 2016-17 (page no: 115)
- CMMRS edition 6, 2016-17 (page no: 116)
- CMMRS edition 6, 2016-17 (page no: 110)
- CMMRS edition 6, 2016-17 (page no: 125)
- CMMRS edition 6, 2016-17 (page no: 117)
- CMMRS edition 6, 2016-17 (page no: 118)
- CMMRS edition 6, 2016-17 (page no: 119)
- CMMRS edition 6, 2016-17 (page no: 120)
- CMMRS edition 6, 2016-17 (page no: 85)
- CMMRS edition 6, 2016-17 (page no: 75)
- Jawetz, Melnick, & Adelberg’s Medical Microbiology Twenty-Seventh Edition (page no: 344)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 343)