

Summary
Treponema pallidum is a thin spirochete that is known for causing syphilis [1]. Other species of this group and the corresponding diseases they cause are the following [2]:
Treponema pallidum pertenue: yaws
Treponema pallidum endemicum: endemic syphilis
Treponema pallidum carateum: pinta
Treponema pallidum is a thin spirochete that is known for causing syphilis [1]. Other species of this group and the corresponding diseases they cause are the following [2]:
- Treponema pallidum pertenue: yaws
- Treponema pallidum endemicum: endemic syphilis
- Treponema pallidum carateum: pinta
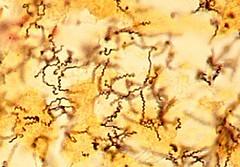
ff treponema pallidum by isis325 is licensed under CC BY 2.0.
Virulence and microbiologic features:
- Treponema pallidum is catalase negative and microaerophilic [1].
- Since it lacks tricarboxylic acid, it relies on host metabolic machinery to meet its amino acids and nitrogenous base requirements. Therefore, it is difficult to culture on an artificial media [1].
- The organism is sensitive to drying and high temperature [3].
- Hyaluronidase can possibly help the perivascular invasion of the organism [4].
- Outer membrane proteins facilitate bacterial attachment with the target cells [4].
- The organism is motile [5] and has devised mechanisms to evade phagocytosis, such as coating itself with host fibronectin [4].
- Unlike some other bacteria, it lacks transposable elements. Therefore, its genetic makeup is unaltered, and the organism is still penicillin-sensitive [3].
Transmission:
- Transmission is mainly through sexual contact [6].
- Vertical transmission can occur in pregnant females [7].
- Skin contact with the infectious lesion during examination can also result in occupational exposure [6].
Disease and complications:
Primary syphilis: The patient may present with a papule, which can manifest up to 90 days following the initial exposure and subsequently evolve into a painless ulcer. The patient may also develop non-tender enlargement of regional lymph nodes. [7]
Secondary syphilis: This stage can develop in untreated patients. Bacteremia results in the systemic spread of the pathogen, which can involve multiple body organs. The patient develops an extensive rash that also involves the oral cavity, as well as the palms and soles. Patients can also develop a highly infectious lesion called condyloma latum in the genital area. Some other clinical findings of this stage include pyrexia, weight loss, and diffuse lymphadenopathy. [8]
Latent syphilis: The patient can become asymptomatic in this stage, and systemic symptoms subside. Some patients may relapse from the latent to the secondary stage, or they may gradually progress to the tertiary phase. Although in the later latent stage, the patient is considered non-contagious, there is still a risk of vertical transmission in pregnant females [8].
Tertiary syphilis: Some possible clinical manifestations of tertiary syphilis are the following:
- Gummatous syphilis: It is characterized by painless granulomatous lesions that can involve skin and bones [8].
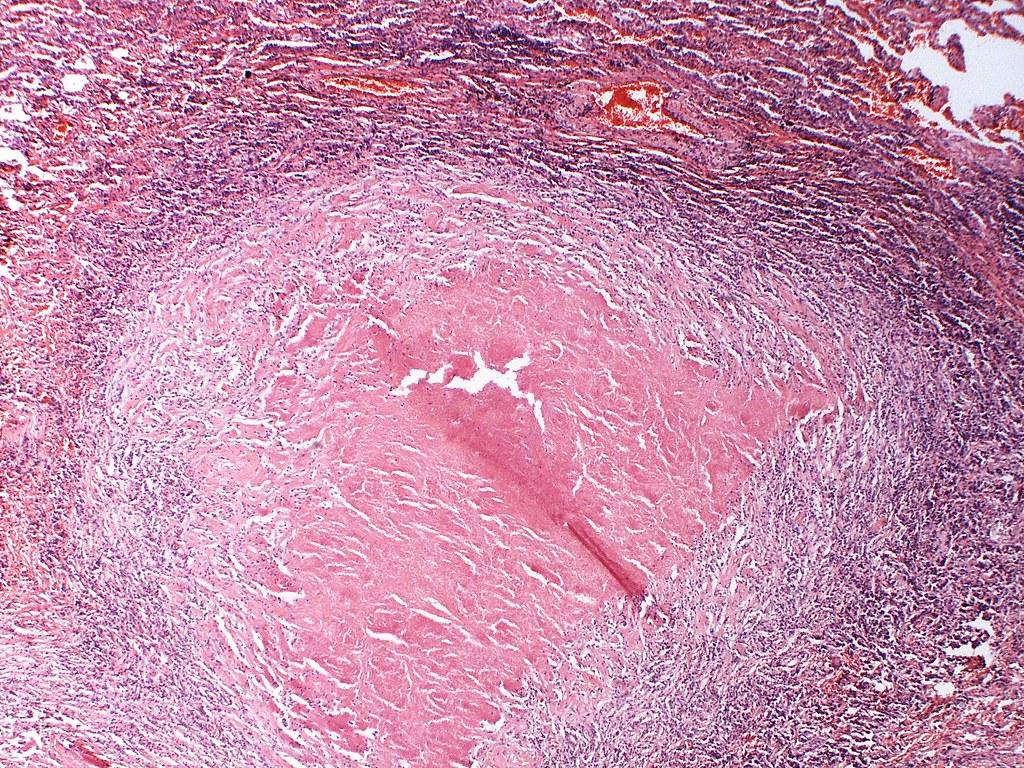
Syphilitic gumma Case 278 by Pulmonary Pathology is licensed under CC BY-SA 2.0.
- Cardiovascular syphilis: The inflammatory response to the bacterium can gradually damage the small blood vessels supplying the aorta, leading to necrosis of the tunica media. Subsequently, the patient may develop aortic aneurysm and aortic dissection. Progression can result in complications such as aortic valve dysfunction or blockage of the coronary arteries. Notably, these complications are not reversible with antibiotic treatment. [8,9]
- Neurosyphilis: Patients with neurosyphilis can be asymptomatic. Other possible clinical manifestations include subacute meningitis with elevated CSF lymphocyte count (unlike other bacterial meningitis in which CSF neutrophil levels are high), meningovascular syphilis, or tabes dorsalis. Tabes dorsalis is due to the involvement of the posterior column, dorsal roots, and dorsal root ganglia. Patients with tabes dorsalis can present with Argyll-Robertson pupil, ataxia, diminished reflexes, and loss of pain and temperature sensations.[9]
- Congenital syphilis: Clinical manifestations of congenital syphilis include lymphadenopathy, hepatosplenomegaly, snuffles, and rash. The affected child can also develop sensorineural deafness, saddle nose deformity, saber shins, mulberry molars, and Htchinson’s teeth. [9]
Diagnostic testing:
- Darkfield microscopy and direct fluorescent antibody tests can help visualize the organism. Darkfield microscopy is not very useful for oral and rectal specimens because these specimens can contain non pathogenic spirochetes. The direct fluorescent antibody test is helpful for oral and rectal specimens. [10]
- Serological tests include:
- Nontreponemal tests (such as venereal disease research laboratory (VDRL) test and the rapid plasma reagin (RPR) tests) are screening tests. Following a positive test result, healthcare providers subsequently confirm it with a treponemal test. Non-treponemal tests can be false positive in pregnant patients or after immunization. [10]
- Treponemal tests include fluorescent treponemal antibody–absorption (FTA-ABS), treponema pallidum particle agglutination (TP-PA) test, or enzyme immunoassays. Patients with AIDS can have a negative treponemal test. [11]
- Polymerase chain reaction (PCR) [10]
References:
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 323)
- CMMRS edition 6, 2016-17 (page no: 133)
- Jawetz, Melnick, & Adelberg’s Medical Microbiology Twenty-Seventh Edition (page no: 323)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 321)
- CMMRS edition 6, 2016-17 (page no: 138)
- CMMRS edition 6, 2016-17 (page no: 128)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 324)
- CMMRS edition 6, 2016-17 (page no: 129)
- CMMRS edition 6, 2016-17 (page no: 130)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 325)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 326)